
 The chewing surfaces of your child’s back teeth are the most likely place for a cavity to form in his or her mouth. If you run your tongue over this portion of your mouth, you’ll notice why: These portions of your teeth are not as smooth as the rest of your teeth. Instead, they’re lined with microscopic grooves known as “pits and fissures,” which trap bacteria and food particles. A toothbrush’s bristles can’t always reach all the way into these dark, damp recesses. This generates ideal circumstances for tooth decay to flourish.
The chewing surfaces of your child’s back teeth are the most likely place for a cavity to form in his or her mouth. If you run your tongue over this portion of your mouth, you’ll notice why: These portions of your teeth are not as smooth as the rest of your teeth. Instead, they’re lined with microscopic grooves known as “pits and fissures,” which trap bacteria and food particles. A toothbrush’s bristles can’t always reach all the way into these dark, damp recesses. This generates ideal circumstances for tooth decay to flourish.
Furthermore, a child’s newly erupted permanent teeth do not have the same level of decay resistance as adult teeth. As teeth age, the hard enamel coating that protects them changes to become stronger. Fluoride, which can be found in toothpaste and some drinking water — as well as dental treatments — can help to strengthen enamel, but it’s difficult to get fluoride into those pits and fissures on a regular basis. Dental sealants, fortunately, are a viable answer to this issue.
Dental sealants are clear plastic resin coatings that smooth up the chewing surfaces of the back teeth and make them decay-resistant. A sealed tooth is significantly less likely to develop a cavity, necessitate more costly dental care in the future, or, most importantly, cause pain to your child.
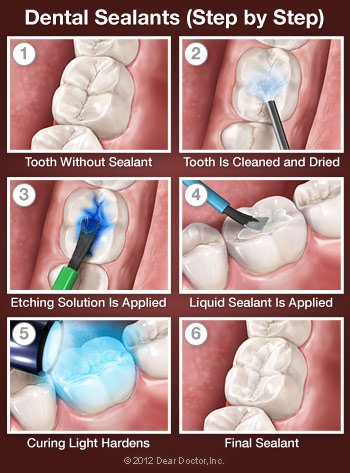
How Dental Sealants Are Placed
You can think of a sealant as a mini plastic filling, though please reassure your child that it doesn’t “count” as having a cavity filled. Because tooth enamel is devoid of nerves, applying a sealant is painless and does not necessitate the use of numbing agents. The tooth or teeth to be sealed are first examined, and any little decay discovered is carefully removed. After that, the tooth will be cleansed and dried. The surface is next treated with a solution that roughens or “etches” it somewhat, allowing the sealing substance to adhere better. After that, the tooth is cleaned and dried one more. The liquid sealant is then painted on the tooth and solidifies in about a minute, sometimes with the assistance of a special curing light. It’s as simple as that!
Taking Care of Your Dental Sealants
Sealed teeth, like unsealed teeth, require the same level of dental hygiene. Your child should continue to brush and floss his or her teeth on a daily basis, as well as undergo professional cleanings on a regular basis. It’s crucial to keep an eye on the sealants for signs of wear and tear, even though they should last for up to ten years. During this period, your child will receive a preventive therapy that has been shown to minimize decay by over 70%.
New parents have plenty to worry about: making sure their baby is healthy and happy, re-arranging their lives around hectic schedules and lost sleep, and figuring out what to do in all sorts of novel situations. There is, however, plenty of assistance available when it comes to your child’s oral health. It all starts when you bring your child in for his or her first dental appointment.
A child’s first checkup should take place by the age of one, according to the American Academy of Pediatric Dentistry. Surprised? You shouldn’t be doing that! Even if only a few baby teeth are visible at that age, there are plenty of things to start working on, including the establishment of healthy habits that will make future dental appointments much more pleasant.
Some children, unfortunately, suffer tooth rot at a young age. We’ll be looking for cavities, but that’s not the only reason to come in early. Reviewing how to properly care for a young child’s mouth, going through your child’s growth stages, and explaining the need of good oral hygiene are all equally vital.
Preparing for the First Dental Appointment
Children have an extraordinary ability to pick up on their parents’ emotions, so if you’re apprehensive about going to the dentist, try not to show it. In most cases, the first visit consists of simply speaking with you and your child, inspecting his or her mouth, and performing oral health evaluations. It’s better to let your child know what to expect ahead of time without making a huge deal out of it. You may even assist them prepare for “the big day” to add to the excitement.
It’s a good idea to carry a soothing toy, a snack, and a spare diaper or two in case your child becomes fussy. If at all possible, leave other children at home so that the new patient receives all of your attention. If that isn’t possible, bringing another adult around might help you focus on your child’s oral health. Filling out documents ahead of time can also save time and effort on the day of the appointment.
The Checkup
When you and your child are both comfortable in the clinic, a sensitive examination of your child’s mouth will be performed to detect any early symptoms of dental problems such tooth decay and to determine the likelihood that your child will acquire the condition in the future. Without drilling, this type of risk assessment can often help prevent — and even reverse — the early stages of tooth disease.
Various methods for maintaining your child’s dental health will be covered. This could include information on how food, eating habits, and oral cleanliness can help prevent tooth decay, which is the most frequent chronic disease in children. This is an essential topic for everyone, but especially so if your child is at risk. A comprehensive explanation will be given if any treatments (such as fluoride) are required. Cleaning and brushing tips will be discussed, and if necessary, a follow-up visit will be made.
Many habits are formed at a young age. That is why “getting it done by age one” is critical. So don’t be hesitant when it’s time for your child’s first visit! You’re going to be glad you came in.

Your child’s infant teeth are in charge of a lot of things. They will not only assist your child bite, chew, and speak correctly until adolescence, but they will also guide the permanent teeth beneath them into perfect alignment. Indeed, one of the primary functions of baby teeth is to create space for adult teeth that will eventually push them out.
At least, that’s how it’s meant to operate; nonetheless, damage or disease might result in the early loss of a baby tooth. When this happens, the permanent teeth on either side of the space that was set aside for another tooth may actually slide into it. This can cause teeth to erupt out of position or to be blocked entirely, and it may result in crowded or crooked teeth.
If your child loses a tooth too soon, a dental appliance can be utilized to keep the space open for the permanent tooth that will eventually replace it. The gadget is known as a “space maintainer” or “space maintenance appliance,” as the name implies. Space maintainers are made of metal or plastic and can be set (cemented) or removable, but their goal is the same in any case: to assist your child grow the best bite possible and avoid the need for braces in the future.
Fixed the appliances are bonded to the teeth next to them. They come in a variety of styles, including: One is made up of a band that wraps around a tooth and then has a wire loop that extends out from the band to hold the space; another is made up of a loop attached to a stainless steel crown that goes over an adjacent tooth. The loop extends just to the point where it reaches the next tooth in either situation. Fixed space maintainers are generally chosen by younger children over removable appliances since they are less simple to fiddle with, break, or misplace.
Removable appliances resemble the sort of retainer used at the conclusion of orthodontic treatment. It can be fitted with a false tooth, which is especially advantageous when the missing tooth is visible in the mouth. Older youngsters are usually capable of handling the responsibility of wearing and caring for this device.
Your child’s space maintainer, whether fixed or detachable, will be custom-made after we take impressions of his or her lips. A space maintainer is worn by a youngster until x-rays show that the tooth underneath is ready to erupt naturally. Anyone who wears a space maintainer should practice good oral hygiene at home and undergo professional dental cleanings on a regular basis.
When one or more permanent teeth are congenitally missing — that is, they have never been — space maintainers can help. Permanent dental implant teeth are commonly advised for adolescents or adults to replace a tooth they were not born with in circumstances like these, which are fairly rare. Dental implants, on the other hand, require precise scheduling because they cannot be placed in a developing youngster. As a result, using a space maintainer with a false tooth on it until jaw growth is complete and an implant can be properly placed is critical. With little timely intervention, we can avert a malocclusion (poor bite) in an easy, non-invasive approach.
 Over the last decade, the number of youngsters diagnosed with Attention Deficit Hyperactivity Disorder (ADHD) has gradually increased. According to a recent study, many children who have been labeled with this ailment may not actually have it; their behavioral issues are caused by sleep-related breathing disorders (SRBD), such as sleep apnea.
Over the last decade, the number of youngsters diagnosed with Attention Deficit Hyperactivity Disorder (ADHD) has gradually increased. According to a recent study, many children who have been labeled with this ailment may not actually have it; their behavioral issues are caused by sleep-related breathing disorders (SRBD), such as sleep apnea.
Over the last decade, the number of youngsters diagnosed with Attention Deficit Hyperactivity Disorder (ADHD) has gradually increased. According to a recent study, many children who have been labeled with this ailment may not actually have it; their behavioral issues are caused by sleep-related breathing disorders (SRBD), such as sleep apnea.
When you think about it, it makes perfect sense: a well-rested human, young or old, can perform much better on a good night’s sleep. Adults and children, on the other hand, are affected differently by a lack of sleep. While tired adults appear sluggish and drowsy, sleep-deprived children, including children with ADHD, are more prone to become hyperactive, uncooperative, and unable to focus.
So what exactly is SRBD?
Recurrent episodes of disrupted breathing during sleep characterize the illness. Soft tissues in the back of the throat, such as the tonsils or the tongue, partially close off the windpipe, obstructing the child’s airway. When air travels through these tissues, they vibrate, creating snoring. It’s usually worse when lying on one’s back because the lower jaw tends to fall back, pushing the tongue in front of the airway.
Sleep apnea is more common in overweight children due to fatty tissue deposits in the soft palate, which reduce the size of the child’s airway.
Is your youngster suffering from a sleep-related respiratory problem? By watching your child sleep, you can gather information to relay to your doctor. Keep an eye out for the following signs:
- Snoring
- Pauses in breathing
- Chronic mouth breathing
- Constant tossing and turning
- Night panics
- Bed-wetting
How is sleep apnea treated in children?
There are various treatments that can be very effective, depending on the cause. Enlarged tonsils and adenoids can be surgically removed.
Continuous Positive Airway Pressure (CPAP) is a therapy that involves using a machine to deliver modest air pressure through a mask worn while sleeping to maintain the airway open.
In some cases, dentistry might help with treatment. The use of a palatal expander, a type of orthodontic appliance, has proven to be beneficial in some circumstances for younger children who are still growing. By gently separating bones that don’t permanently fuse together until puberty, a palatal expander gradually extends the roof of the mouth (palate). It’s most commonly done to make extra space for crowded teeth, although it can also improve ventilation.
Oral Appliance Therapy can sometimes help older children who have stopped growing (OAT). This entails sleeping with a custom-made oral appliance that repositions the jaw during sleep, keeping the tongue away from the back of the throat and therefore lowering the risk of obstruction.
The first step is to identify what is preventing your child from obtaining the restorative sleep that is so important for his or her health and well-being. You will need to see a skilled specialist in order for this to happen and for your child to receive the finest therapy possible.
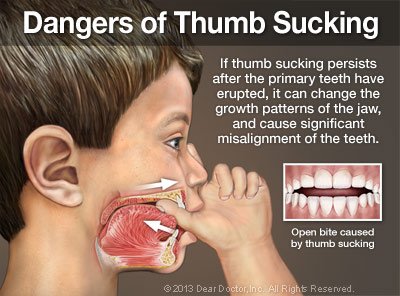 Sucking on a thumb or finger is a completely normal habit that some babies develop even before they’re born. It’s relaxing, yet it also encourages newborns to interact with and explore their surroundings. However, if a child’s sucking habits continue past the age of three, bite difficulties may develop.
Sucking on a thumb or finger is a completely normal habit that some babies develop even before they’re born. It’s relaxing, yet it also encourages newborns to interact with and explore their surroundings. However, if a child’s sucking habits continue past the age of three, bite difficulties may develop.
The top teeth grow to overlap the lower teeth in a normal bite. The pressure of a thumb, finger, or pacifier sitting on the gums, on the other hand, might obstruct natural tooth eruption and even jaw growth. Some thumb-suckers develop a “open bite,” which means that when a youngster bites together, the upper and lower teeth do not overlap, leaving an open gap between them. That’s why, while we don’t want to intervene too soon, we should absolutely keep a watch on thumb sucking.
Breaking the Habit
It’s crucial to remember that most youngsters between the ages of 2 and 4 stop sucking their thumbs on their own. So, if you want your child to cease, the first thing you should do is ignore them. Pacifiers are typically given up faster than thumbs or fingers. If your youngster refuses to stop when it’s time, positive reinforcements are more effective than negative reinforcements (e.g., putting a bitter substance on the thumb). Here are some ideas to get you started:
- Praise & Reward. Explain why it’s so vital for your child not to suck her thumbs and come up with a way to thank her for not doing so — as long as it’s not with tooth-harming sweets! Stickers or a fun activity might be appropriate. When you detect a thumb in your child’s mouth, always offer gentle reminders rather than scolding, and congratulate her when she stops.
- Comfort & Distract. Thumb sucking is triggered in different ways by different children. Is it something your youngster does when he or she is stressed or bored? If that’s the case, some additional hugs or an activity to keep those little hands occupied might be beneficial.
- Get Creative. You are the most knowledgeable about your child. Perhaps there is a method that he would find very motivating. You could, for example, attach his pacifier to a helium balloon and mail it to the Tooth Fairy. She can slip a special present beneath his pillow when she receives it!
- Get Help. Dentistry can help if your child sucks her thumb, fingers, or a pacifier. Sometimes all it takes is a quick talk with a caring dental practitioner to explain how it will help her teeth kick the habit. If necessary, she can be placed with a tongue crib (View Example), an unique oral appliance that physically prevents thumb sucking and can typically be broken in a few months.
Thumb sucking is only one of the reasons why it’s critical to keep your child’s dentist appointments on a regular basis, beginning at the age of one. You and your child can also learn excellent oral hygiene habits to help prevent tooth decay at these appointments. In the meantime, your child’s dental development and growth will be watched. Though orthodontics can usually correct bite abnormalities caused by sucking behaviors, we’d prefer to help you avoid this cost if at all feasible!
 Fluoride is a naturally occurring mineral that is necessary for optimal tooth development and tooth decay prevention. Tooth decay may still be a serious problem in many areas across the United States, although it is significantly less widespread than it would have been if public water supplies were not fluoridated. As a result, the major pediatric dental and medical groups support water fluoridation at the current recommended level of 0.70 parts per million (ppm). Fluoridated water is also one of the most significant health successes of the twentieth century, according to the federal Centers for Disease Control and Prevention (CDC).
Fluoride is a naturally occurring mineral that is necessary for optimal tooth development and tooth decay prevention. Tooth decay may still be a serious problem in many areas across the United States, although it is significantly less widespread than it would have been if public water supplies were not fluoridated. As a result, the major pediatric dental and medical groups support water fluoridation at the current recommended level of 0.70 parts per million (ppm). Fluoridated water is also one of the most significant health successes of the twentieth century, according to the federal Centers for Disease Control and Prevention (CDC).
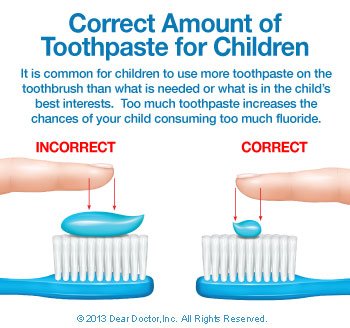
Of course, fluoridated water is not available to everyone. That’s why a fluoride supplement and/or the use of toothpastes and other items containing this crucial mineral are frequently recommended for your youngster. Because too much fluoride can harm children, it’s recommended to get professional guidance before using any fluoride-containing substance.
How Fluoride Helps Kid’s Teeth
The protective outer layer of teeth, called enamel, is often subject to attacks from acids. These can come directly from acidic meals and beverages, such as sodas and citrus fruits, or indirectly through a middleman: decay-causing bacteria that produce acid from sugar already present in the mouth. These bacteria concentrate in dental plaque and feed on sugar left in your child’s mouth after brushing. When bacteria metabolize (break down) sugar, acids are produced that can chip away at tooth enamel. Cavities are generated in this manner. Fluoride becomes a component of the crystalline structure of tooth enamel, hardening it and making it more resistant to acid assault when it is present. Fluoride can even assist in the healing of tiny cavities that have already developed.
Delivering Fluoride to the Teeth
Fluoride in drinking water or supplements can be absorbed by children’s developing permanent teeth. Fluoride can be applied topically to a tooth after it has erupted (on the surface). One strategy to ensure that your children’s teeth receive beneficial fluoride exposure on a daily basis is to use a fluoride-containing toothpaste. For children ages 2 to 6, we recommend using only a pea-sized amount, and for children under two, just a tiny smear. Fluoride should not be given to babies under the age of six months. Topical fluoride applications painted directly onto your child’s teeth and allowed to sit for a few minutes for optimal efficiency are a very excellent technique to provide fluoride to the teeth.
How Much Is Too Much?
Enamel fluorosis is a disorder characterized by a streaked or mottled look in teeth that have been over-exposed to fluoride when they form beneath the gum line. Mild fluorosis appears as small white dots that are difficult to discern. The discolouration might be deeper and have a pitted texture in more severe occurrences (which are uncommon). Although the condition is not hazardous, it may require cosmetic dental treatment in the future. Tooth decay, on the other hand, is hazardous to your child’s health and, in extreme situations, can be quite unpleasant.
By the time a child is about 9 years old, all of his or her permanent teeth have fully developed, the risk of fluorosis has passed. Because fluoride exposure is cumulative, all sources your child comes into contact with should be assessed, including powdered infant formula combined with fluoridated tap water. While caution is urged, ignoring the benefits that this crucial mineral can provide to your child’s teeth — and overall health — would be a mistake.















